
The GLP-1 Plateau Is a Diagnostic Moment, Not a Failure
Every practitioner working with GLP-1 receptor agonists has seen the same trajectory. The first three to six months are remarkable. Patients lose weight that has resisted every prior intervention. Inflammatory markers fall. A1c improves. Energy returns. And then, somewhere between month six and month fourteen, the scale stops moving. The patient panics. They ask if the medication has stopped working. They ask for a higher dose, a different molecule, a stack.
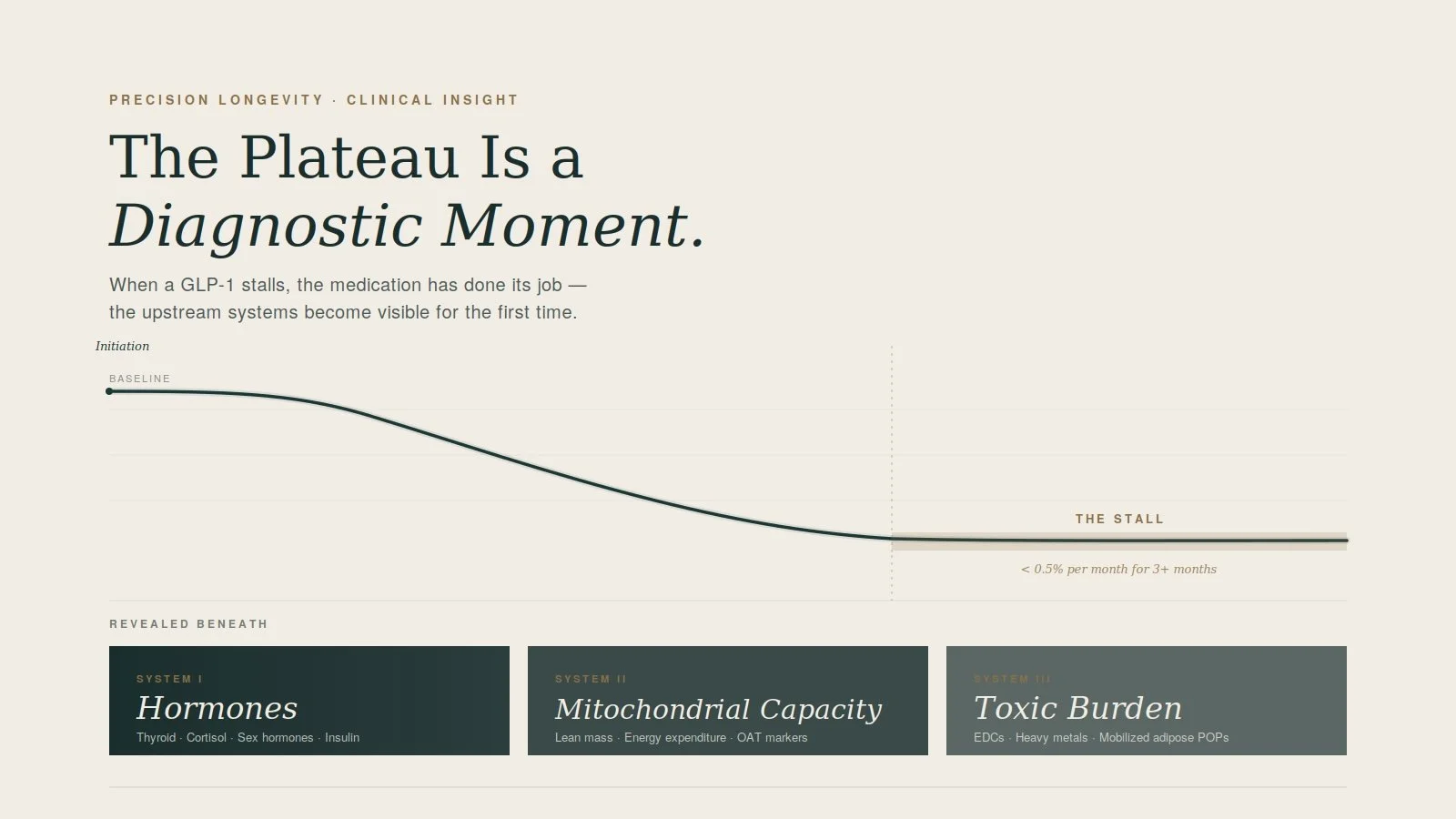
Here is what I tell them, and what I want every clinician reading this to internalize: the plateau is not the failure. The plateau is the most useful diagnostic event of the entire treatment course.
It is the moment the medication has done what it can do, and what is left is the upstream biology the medication was masking. If you read the plateau correctly, you stop chasing dose escalations and start asking the question your patient was avoiding when they came to you in the first place — which of their underlying systems is failing, and what does it take to restore it.
What "Plateau" Actually Means
Before any workup, define the term. A true plateau is less than 0.5% body weight change per month for at least three months on a stable, therapeutic dose with documented adherence. Anything before that is metabolic adaptation — a normal, biologically defended response to weight loss — and not a clinical signal.
Once a patient meets that threshold, you are no longer working with a normal adaptation curve. You are working with a body that has run out of compensatory capacity in one or more upstream systems. That is what needs to be diagnosed.
What the Newest Research Tells Us
Two papers published in the last eighteen months reshaped how I work this up.
The first is a September 2025 paper in Cell Reports Medicine from the McMaster group, which made the mechanism of GLP-1 plateau and rebound substantially clearer. GLP-1 receptor agonist therapy reduces lean muscle mass and triggers adaptive thermogenesis — a measurable downshift in resting energy expenditure that is disproportionate to the weight lost. In plain terms, the patient's metabolic rate drops faster than their body composition would predict, and the muscle they have lost cannot defend the lower set point. This reframes the plateau from an appetite problem into an energy expenditure problem, and it tells you that body composition assessment is no longer optional.
The second is a 2024 systematic review in Obesity Reviews on environmental contaminants and weight loss resistance. The findings are striking. Endocrine-disrupting chemicals — phthalates, parabens, organophosphates, persistent organic pollutants — directly disrupt thyroid hormone, estrogen signaling, insulin sensitivity, and, critically, GLP-1 signaling itself. The mechanism that explains the timing is the part most practitioners have not internalized: persistent organic pollutants are stored in adipose tissue. When your patient loses fat, those compounds are mobilized into circulation, where they suppress the very pathways the medication is trying to activate.
Read those two findings together and the plateau makes mechanistic sense. The patient's own fat loss is generating an internal toxic burden that suppresses mitochondrial output, thyroid conversion, and GLP-1 signaling, while simultaneously losing the muscle mass that would otherwise defend metabolic rate. The medication has not stopped working. The upstream systems have stopped compensating.
The Three-System Workup
When a patient hits a true plateau, I run three categories of testing. Each interrogates a different upstream mechanism, and each tells you something the others cannot.
Hormones first. The minimum panel is free T3, free T4, reverse T3, TSH, four-point cortisol (salivary or DUTCH), fasting insulin with HOMA-IR, leptin, adiponectin, and a full sex hormone panel — estradiol, progesterone, total and free testosterone, SHBG, DHEA-S. In women over forty, perimenopausal hormonal shifts are one of the most under-recognized drivers of GLP-1 plateau, and the timing often coincides almost exactly with when the medication appears to "stop working." In men, declining testosterone and rising SHBG produce the same phenomenon by a different mechanism. Reverse T3 deserves particular attention — adaptive thermogenesis is partly mediated by increased T4-to-rT3 conversion, and standard thyroid panels miss it.
Organic acids next. An organic acids test is one of the highest-yield investigations available at plateau because it interrogates four systems simultaneously. Krebs cycle intermediates and fatty acid oxidation markers tell you whether mitochondrial output is the rate-limiting step. Detoxification markers — pyroglutamic, orotic, sulfate — tell you whether glutathione demand is exceeding supply, which is what you would expect if mobilized adipose toxins are overwhelming Phase II conjugation. Neurotransmitter metabolites tell you about the dopamine and serotonin pathways that GLP-1 modulates and that often shift at plateau. Microbial markers tell you about dysbiosis, which independently drives metabolic dysfunction. One test, four upstream systems, and almost always actionable findings.
Toxicity panel third, and not optional in this population. Urinary environmental toxin testing for glyphosate, phthalates, parabens, organophosphates, and VOCs, plus a heavy metals panel including mercury, arsenic, cadmium, and lead. The clinical question this answers is why the systems on the first two panels are failing. If the hormone panel shows low free T3 with elevated reverse T3, and the OAT shows mitochondrial sluggishness and high detox demand, the toxicity panel usually closes the loop.
A Sequenced Course of Action
What I do once the results return depends on what they show, but the protocol skeleton is consistent.
If lean mass loss is the dominant finding on body composition assessment, the intervention is resistance training and protein optimization before anything else. The Cell Reports Medicine data is clear that muscle is the lever. I target 1.0 grams of protein per pound of goal body weight, distributed across three to four feedings, paired with progressive resistance training at least three days per week. Creatine monohydrate at three to five grams daily is one of the most evidence-supported additions. Nothing else on this list will work durably if muscle continues to decline.
If hormone dysfunction is driving the plateau, treat it directly. Subclinical hypothyroidism gets a therapeutic trial. Perimenopausal patients with symptomatic estrogen and progesterone decline are candidates for hormone therapy with a properly trained clinician. Cortisol dysregulation gets addressed through adaptogens, sleep architecture, and circadian work — not stimulants, which often worsen the picture.
If the OAT shows mitochondrial dysfunction, the protocol becomes targeted: CoQ10 or ubiquinol at therapeutic doses, acetyl-L-carnitine, alpha-lipoic acid, magnesium glycinate, and B-complex with active forms. Most patients respond within six to twelve weeks if mitochondrial support is the missing piece.
If the toxicity panel is positive, slow the weight loss intentionally and front-load detoxification capacity before continuing. This is counterintuitive to patients but mechanistically essential — pushing further fat loss while detox pathways are saturated mobilizes more toxins into circulation and worsens the plateau. Glutathione precursors (NAC, glycine), binders matched to the specific toxic burden, sauna therapy when tolerated, increased fiber for biliary recirculation, and aggressive hydration. Consider holding the GLP-1 dose constant rather than escalating during this phase.
Across all four scenarios, body composition reassessment at twelve weeks tells you whether the protocol is working. If lean mass is stable or rising, basal metabolic rate is improving, and the patient is symptomatically better even before the scale moves, the plan is correct. The scale will follow.
The Reframe
The most important shift is what you tell the patient at the plateau visit. The medication has not failed. Their body has not failed. What has happened is that the GLP-1 has done its job — it has reduced the load on the systems that were overwhelmed enough to require pharmacological help — and now those systems are visible for the first time. The plateau is the moment precision medicine actually starts.
Patients who understand this stay engaged. Patients who do not understand it ask for a higher dose, a different drug, or a different doctor. The framing is the intervention before the intervention.
GLP-1 receptor agonists are one of the most important pharmacological tools we have. They are also revealing, for the first time at population scale, exactly which upstream systems modern bodies cannot maintain on their own. The clinicians who learn to read the plateau as the diagnostic moment it is will get durable outcomes. The ones who treat it as a dose problem will not.