
The Four Hingepins: The Biological Drivers Underneath Every Longevity Protocol That Actually Works
Why the downstream diseases almost never respond durably to downstream protocols — and what happens when you intervene at the four points of biological leverage instead.
Why "Upstream" Is Not Just a Slogan
Every precision longevity practitioner has said some version of it. "We work upstream." "We treat the root cause." "We ask why, not just what." These phrases have become so common they have started to lose meaning, even to the practitioners using them.
Here is what upstream actually means, mechanistically. It means there are specific biological systems — not metaphors, not philosophies, but measurable cellular and tissue-level functions — that determine whether the downstream disease takes hold, progresses, stalls, or reverses. When those systems are working, the body does the repair work on its own. When those systems are broken, no amount of downstream intervention will fully compensate. You can manage the symptoms, sometimes impressively, but you cannot restore the underlying biology.
The Four Horsemen are downstream. ASCVD, cancer, neurodegenerative disease, metabolic dysfunction — these are the outcomes. By the time they are clinically obvious, years or decades of upstream dysfunction have already happened. Treating them at the Horsemen level means chasing disease that has already taken root.
The Four Hingepins are upstream. They are the four biological systems on which the Horsemen turn. Fix the Hingepins and the Horsemen lose their foothold. Miss the Hingepins and every downstream protocol you design will eventually hit a ceiling you cannot understand.
This is the architecture inside the Woods Method. It is also the architecture inside every Body MAX Harmonics BOT output. This essay walks through each of the four, in the order I typically look for them in clinical practice.
Hingepin One: Mitochondrial Insufficiency
Every cell in the human body either has working mitochondria or it does not. When it does not, nothing else you do upstream will land.
Mitochondrial insufficiency is the quiet backdrop to an enormous amount of what presents as fatigue, brain fog, cognitive decline, exercise intolerance, post-viral syndromes, and the general sensation of "being well but not really well" that brings people into longevity practices in the first place. It is also, not coincidentally, the mechanism underneath most of what we currently call neurodegeneration. Parkinson's disease is substantially a disorder of dopaminergic neuron mitochondria. Alzheimer's disease has a documented mitochondrial component well before amyloid and tau become the visible story. The chronic fatigue that follows viral illness is, at the cellular level, a mitochondrial shutdown that the rest of the system reorganizes itself around.
The diagnostic tools here are better than most practitioners realize. Organic acids testing can flag specific mitochondrial pathway dysfunction — the Krebs cycle intermediates, the fatty acid oxidation markers, the evidence of blocked energy production at specific enzymatic steps. Metabolomic panels add resolution. Genetic variants in mitochondrial biogenesis and antioxidant defense add context. The information is there if you know to ask for it.
The intervention architecture is equally specific. Urolithin A as a mitophagy activator. Coenzyme Q10 in reduced form. Nicotinamide riboside and its cousins. Plasmalogen precursors. Pyrroloquinoline quinone. Photobiomodulation. Careful mitochondrial nutritional support built on the specific pathway dysfunction the testing revealed. This is not the "take some CoQ10" school of mitochondrial support. It is targeted cellular energy restoration as a first clinical move, not an afterthought.
If you do not address mitochondrial insufficiency first — or at minimum alongside everything else — the client does not have the cellular energy to execute the rest of your protocol. This is why well-designed longevity interventions sometimes fail for reasons that seem invisible. The scaffolding was missing.
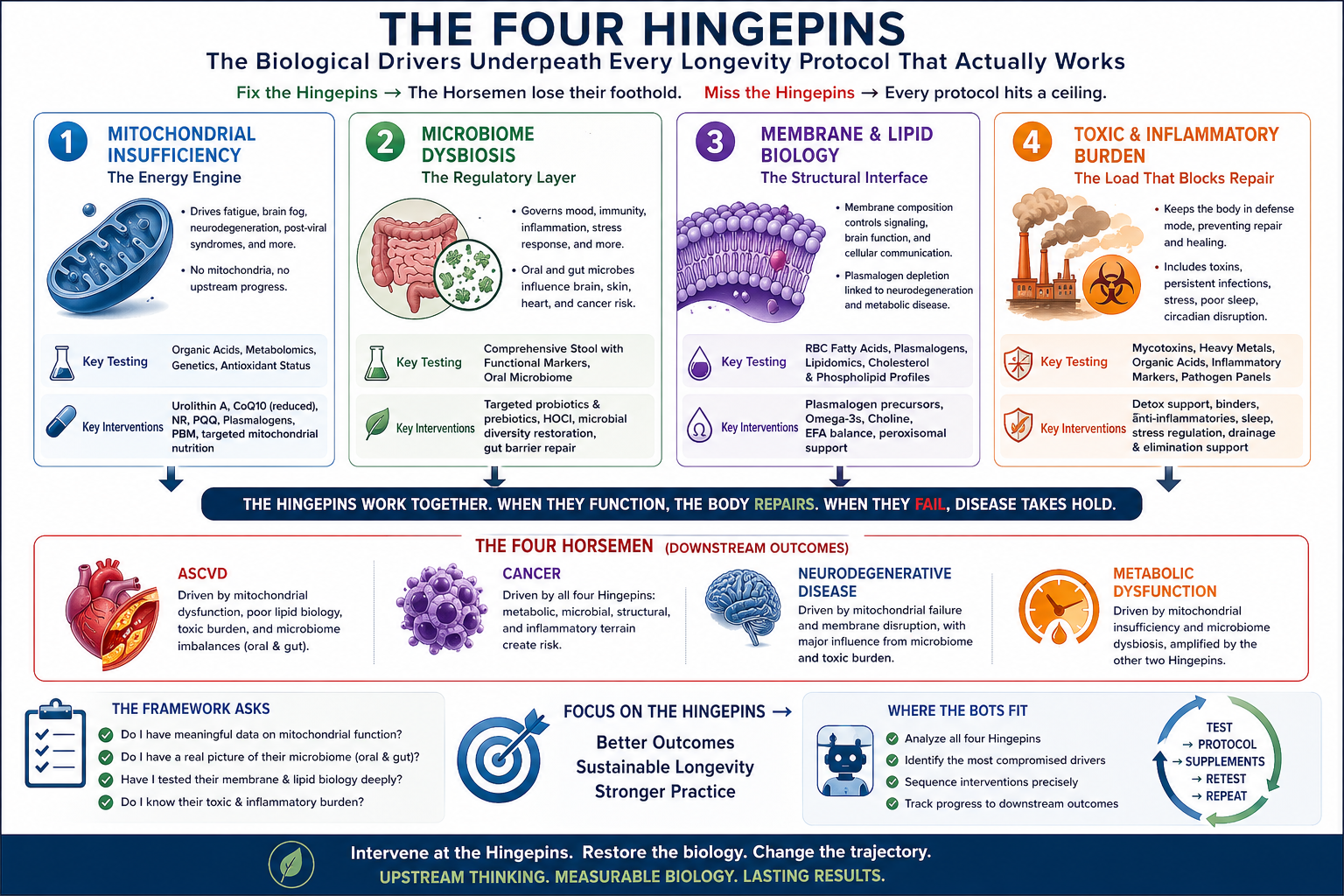
Hingepin Two: Microbiome Dysbiosis
If mitochondria are the energy layer, the microbiome is the regulatory layer. And the regulatory layer turns out to govern a remarkable proportion of the conditions we have spent a century trying to treat from downstream.
The gut microbiome is now understood to bidirectionally co-regulate the dopamine, serotonin, GABA, and glutamate circuits that substances of abuse target — which is why addiction is increasingly reconceptualized as a gut-brain disorder and not exclusively a central nervous system condition. It regulates the HPA axis response to psychosocial stress. It determines whether tryptophan gets metabolized toward serotonin or diverted into the kynurenine pathway that is disrupted in depression. It produces somewhere between 90% and 95% of the body's serotonin. Specific probiotic strains have direct neuropharmacological mechanisms, modulating GABA receptor expression via the vagus nerve.
The oral microbiome is its own regulatory hub. Two-sample Mendelian randomization has now established causal relationships between gut microbiota and four common inflammatory skin diseases — eczema, acne, psoriasis, and rosacea. Fusobacterium nucleatum and Porphyromonas gingivalis have been identified in pancreatic ductal adenocarcinoma tissue and in breast tumors, with bacterial load correlating with tumor size and progression. The estrobolome — the gut microbial genes that mediate estrogen conjugation — links dysbiosis to estrogen-driven cancers through elevated beta-glucuronidase activity.
This is not soft nutritional thinking. This is upstream oncology, upstream psychiatry, upstream dermatology, all mediated by a regulatory system most conventional medicine does not yet know how to interrogate.
The clinical implications are concrete. Comprehensive stool testing with functional markers — not just pathogen panels. Oral microbiome consideration in cancer prevention. HOCl-based interventions where the evidence supports them, particularly for the oral-origin pathobionts linked to systemic disease. Structured microbiome restoration sequencing rather than the spray-and-pray probiotic approach. This is the second Hingepin, because it is the second place most downstream disease is written.
Hingepin Three: Membrane and Lipid Biology
The third Hingepin is the one most practitioners have not been trained to see at all.
Every cell membrane in the human body is built from specific phospholipids in specific ratios. Those ratios are not fixed. They are the product of what the client eats, what their body absorbs, what it can synthesize, and what gets degraded under oxidative and inflammatory pressure. When membrane composition goes wrong — when plasmalogens deplete, when omega-3 to omega-6 ratios distort, when cholesterol content shifts away from healthy cellular architecture — every signaling system that depends on those membranes begins to malfunction.
This is not an abstract concern. Plasmalogen depletion is now documented in Alzheimer's disease, Parkinson's disease, and across the metabolic syndrome cluster. The brain is 60% lipid by dry weight; its membranes are chemically complex in ways that generic "good fats" advice does not begin to capture. Neuronal function, synaptic plasticity, mitochondrial membrane function, and immune receptor behavior all depend on membrane chemistry we are only now beginning to test for and intervene on precisely.
The diagnostic toolkit is expanding rapidly. Plasmalogen assays. Red blood cell fatty acid panels with distinct interpretation for tissue versus membrane status. Advanced lipidomics. The interventions include plasmalogen precursors, targeted omega-3 dosing calibrated to actual baseline, and attention to the enzymatic machinery — peroxisomal function specifically — that builds these lipids in the first place.
If a client has been through the longevity sequence and plateaued — addressed gut, addressed mitochondria, addressed inflammation, addressed hormones — and is still not quite well, the membrane layer is often where the answer is hiding. This is the Hingepin that separates serious practice from superficial practice.
Hingepin Four: Toxic and Inflammatory Burden
The fourth Hingepin is the one every practitioner has heard of and most still underestimate.
Environmental toxicant burden, persistent infection, chronic activation of the immune system — these keep the body in chronic defense instead of chronic repair. Until the load is reduced, the repair mechanisms on the other three Hingepins cannot fully engage. Mitochondrial support stalls because the cell is still burning energy on defense. Microbiome rebuilding stalls because the inflammatory environment keeps rejecting the work. Membrane rebuilding stalls because the oxidative pressure keeps degrading what you build.
This includes the obvious — heavy metals, mycotoxins, PFAS, pesticide residues, persistent viral reactivation, chronic low-grade infections at the oral or gut mucosal level. It also includes less obvious sources: endogenous inflammatory load from unresolved emotional or traumatic stress, sleep disruption that keeps the glymphatic system from clearing, circadian rhythm disorder that leaves the HPA axis stuck in activation.
The clinical work here is sequencing. You do not begin with aggressive detoxification in a client whose elimination organs are not ready. You prepare — drainage pathways, binders, liver support, bowel regularity, kidney hydration — before you mobilize. You address the source alongside the clearance. And you recognize that "toxic burden" is not a diagnosis; it is a physiological state with a measurable load, a measurable rate of clearance, and a measurable tolerance.
How the Hingepins Connect to the Horsemen
Every Horseman is driven by some combination of these four Hingepins. The specific weighting differs by disease, but the pattern is consistent.
ASCVD is driven primarily by mitochondrial insufficiency (endothelial cells are metabolically demanding), membrane and lipid biology (the atherogenic particles are, in the end, lipid biology gone wrong), and toxic/inflammatory burden (the inflammation that drives the plaque formation). The microbiome contributes through the oral-cardiovascular axis and the gut-cardiovascular axis mediated by TMAO and other microbial metabolites.
Cancer risk is driven by all four Hingepins simultaneously. Mitochondrial dysfunction is increasingly understood as central to the metabolic theory of cancer. Microbiome dysbiosis contributes to multiple cancer types through specific mechanisms. Membrane biology governs the cellular signaling that controls proliferation and apoptosis. Toxic burden creates the oxidative and inflammatory terrain in which malignant transformation becomes likely.
Neurodegenerative disease is driven dominantly by mitochondrial insufficiency and membrane biology (the brain is a mitochondria-dense, lipid-rich organ) with major contributions from microbiome (the gut-brain axis) and toxic burden (particularly unresolved inflammation and environmental neurotoxins).
Metabolic dysfunction is driven dominantly by mitochondrial insufficiency (mitochondria are where metabolism happens) and microbiome (the gut regulates metabolic signaling broadly) with major contributions from the other two.
This is why a longevity protocol designed at the Horseman level alone hits ceilings. You can manage ASCVD markers impressively with statins, diet, and exercise — and still fail to reverse the underlying biology because the mitochondrial, membrane, and inflammatory Hingepins were never addressed. You can produce good-looking cancer prevention checklists and still miss the patient whose microbiome is the actual driver. You can prescribe the correct cognitive longevity protocol and watch it stall because the membrane biology never got the attention it needed.
The Hingepins are where the protocol decisions are actually made. The Horsemen are where the protocol decisions are measured.
What the Framework Asks of the Practitioner
The Four Hingepins Framework is not a checklist. It is a demand for a specific quality of attention — the willingness to keep asking "what is upstream of this?" until you arrive at one of these four biological systems, and then to intervene there, with the tools the evidence actually supports.
For every complex client in your active caseload, ask yourself these four questions.
Do I have meaningful data on their mitochondrial function, or am I assuming it is fine because their energy is good on most days?
Do I have a real picture of their microbiome — oral and gut — or am I working from a stool test ordered two years ago?
Have I ever tested their membrane and lipid biology at a level deeper than a standard lipid panel? Do I know whether their plasmalogens are depleted?
Do I know what their toxic and inflammatory burden is, or am I interpreting a vague sense of fatigue as "just stress"?
Most practitioners who run this audit honestly find that two or three of those answers are uncomfortable. That is not a failure of intelligence or effort. It is the signature of trying to do upstream work with downstream-level data.
Where the BOTs Fit
This is slow work when done by hand. Cross-referencing four Hingepins' worth of testing, across a full caseload, interpreting the patterns that emerge between them, and designing protocols that intervene on all four in the correct sequence — this is the invisible second job that drives practitioners out of precision longevity practice after three or four years.
The Body MAX Harmonics clinical BOTs were built around exactly this framework. Every BOT output reasons across all four Hingepins. Every protocol identifies which Hingepins are most compromised in this specific client and sequences the interventions accordingly. Every retest cycle checks whether the Hingepin work is landing on the downstream Horsemen markers.
The BOTs do not replace the upstream thinking. They carry it — at the scale and speed a working clinical practice actually requires.
The upstream thinking was always the hard part. The scaffolding around it does not have to be.
Dr. Lily Woods, PhD is the founder of Body MAX Harmonics and the designer of the Woods Method protocol system. Body MAX Harmonics is a wellness education program for licensed and certified practitioners. Materials provided are wellness education frameworks applied at the discretion of the practitioner within their own scope of practice.