
Testing, Protocol, Retesting: The Clinical Cadence That Builds Both Outcomes and Practice Economics
Why the practices that deliver the best patient results are also, not coincidentally, the most financially sustainable — and how to engineer the rhythm that makes both possible.
The Two Practice Problems Every Precision Practitioner Faces
Practitioners who build their work around precision medicine typically run into two problems at once.
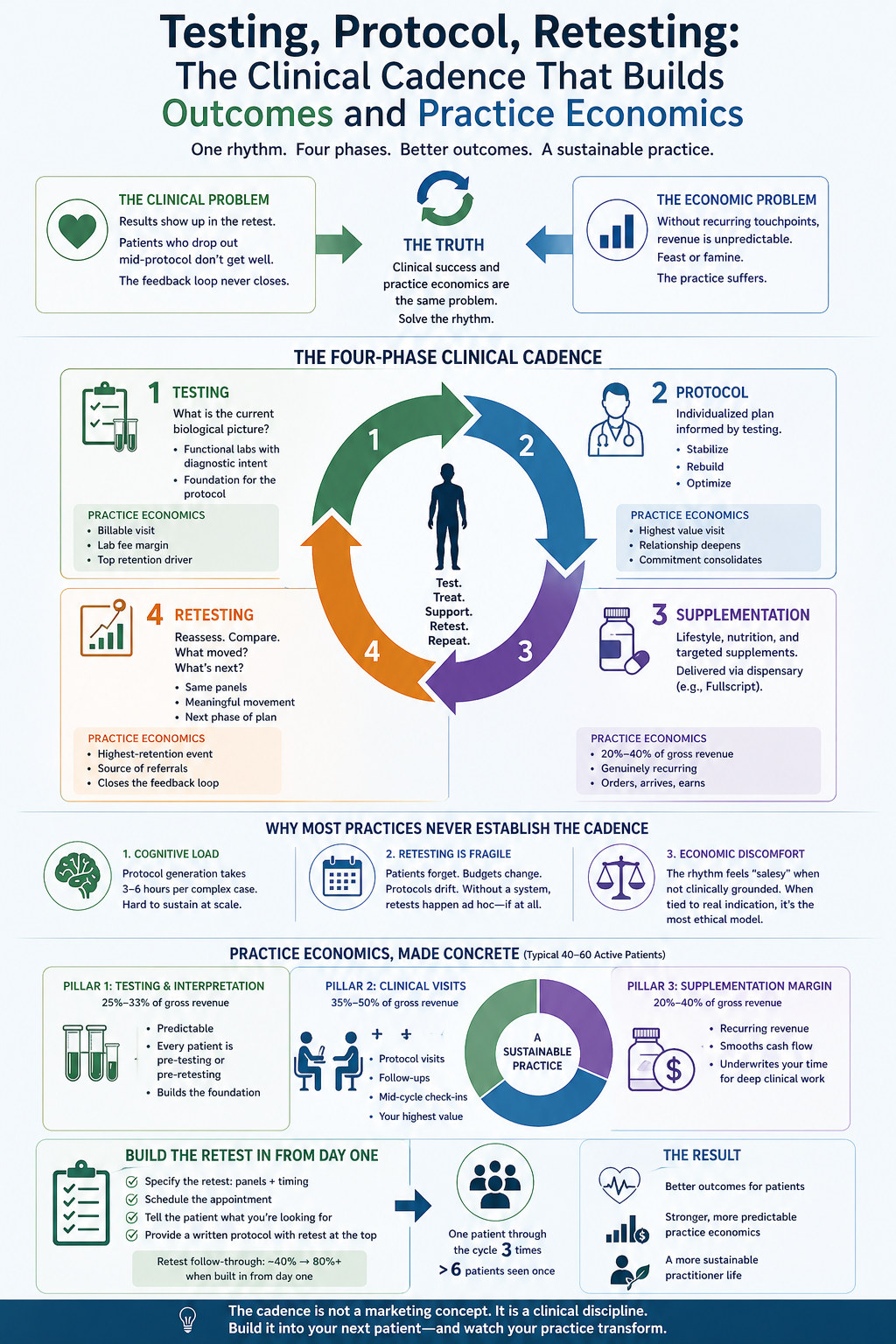
The first is clinical. Complex patients require sustained engagement over months, not single visits. Results show up in the retest, not in the follow-up phone call. Patients who drop out mid-protocol do not get well, and the practitioner cannot tell whether the work was succeeding because the feedback loop never closed.
The second is economic. Cash-pay precision practices depend on a practitioner's ability to create recurring touchpoints — visits, supplementation, testing — that generate predictable revenue. Without that rhythm, the practice lurches between feast and famine, and the practitioner ends up spending their evenings prospecting for new patients instead of deepening the work with existing ones.
What is interesting is that these are not two problems. They are the same problem. The practices that solve the clinical problem — by building a structured rhythm of testing, protocol, supplementation, and retesting — also solve the economic problem, because that rhythm naturally produces the recurring engagement a sustainable practice requires. The practices that leave the clinical rhythm unstructured simultaneously leave the economics unstructured, and both suffer.
This essay is about the specific cadence that I have seen work, why it works, and how to implement it without turning your practice into an extractive supplementation business.
The Four-Phase Clinical Cadence
A well-structured precision practice cycles every patient, every six to twelve months, through the same four-phase rhythm. Each phase has a clinical purpose and a corresponding practice economics purpose. Neither is optional.
Phase one is testing. The patient arrives, or returns from their prior cycle, and the clinical question is the same: what is the current biological picture? Functional labs — stool, organic acids, metabolomics, nutrient panels, hormones, fatty acids, whatever the clinical presentation indicates — are ordered with specific diagnostic intent, not by default. The practice economics corollary: testing creates a billable clinical encounter, a lab fee margin if your model includes it, and the foundation for the protocol revenue that follows. Testing is also the single most important retention tool in your practice. Patients who have recently tested are patients who are engaged.
Phase two is protocol. The practitioner, now informed by the testing, designs an individualized protocol. Stabilization first. Rebuilding second. Optimization third. The protocol is presented with clinical reasoning, not as a list of supplements. The patient understands not only what they are doing but why. The practice economics corollary: the protocol visit is the most valuable touchpoint in your cycle, both for the patient and for your practice. It is where the relationship deepens, where the patient's commitment consolidates, and where the recurring supplementation begins.
Phase three is supplementation. The protocol is executed through a combination of lifestyle, nutrition, and targeted supplementation — routed through a dispensary platform like Fullscript, which handles the logistics and generates margin without requiring the practitioner to warehouse or ship product. The patient orders; the practice earns; the supplement arrives; the protocol runs. The practice economics corollary: done well, dispensary supplementation is typically 20% to 40% of a precision practice's gross revenue, and it is genuinely recurring — patients who are mid-protocol reorder on schedule without any additional sales effort from the practitioner.
Phase four is retesting. At a clinically appropriate interval — usually eight to sixteen weeks, depending on the protocol — the patient returns for the retest. The same panels, run again, interpreted in the context of the intervention. What moved. What did not. What the next phase of protocol should address. The practice economics corollary: the retest is the single highest-retention event in a precision practice. Patients who complete a retest with meaningful movement on their labs become the source of your referrals for the next year. Patients who never retest drop out, and the practice has no way to know whether the work was succeeding.
The cadence compounds. One patient, run through this cycle three times in eighteen months, represents substantially more revenue, substantially more clinical depth, and substantially more likelihood of referral than six patients each seen once. The practice that masters the cadence serves fewer patients at greater depth and produces better outcomes, better economics, and a more sustainable practitioner life simultaneously.
Why Most Precision Practices Never Establish the Cadence
If the cadence is this powerful, why do most precision practices not run it?
There are three reasons, and they are the reasons the cadence looks easy on paper and proves difficult in practice.
The first reason is the cognitive load of protocol generation. Phase two — the protocol visit — is where the practitioner spends three to six hours on a complex patient. Interpreting the panels, cross-referencing the findings, sequencing the interventions, writing the protocol in a way the patient can actually execute. Do this for forty patients and the evenings disappear. Skip the depth, hand the patient a generic template, and the outcomes suffer and the cadence breaks down because there is nothing meaningful to retest against.
The second reason is the difficulty of consistent retesting. Retests are clinically essential and logistically fragile. Patients forget. Patients run out of budget. Protocols drift off-schedule. Practitioners who have not built retesting into the original protocol — including timing, specific panels, and patient commitment — find that retests happen ad hoc, if at all. Without a system, the retest phase silently erodes.
The third reason is a subtle but important one: practitioners trained in functional medicine often feel uncomfortable with the recurring economic rhythm of this work. The concern is understandable. Nobody wants to run a supplementation business dressed up as a medical practice. The concern is also resolvable. The rhythm is not extractive when it is clinically indicated. Testing that genuinely informs the protocol is clinical. Protocol supplementation that is actually being used is clinical. Retesting at a clinically appropriate cadence is clinical. What makes the rhythm extractive is divorcing it from clinical indication — selling supplements that are not part of a coherent protocol, running testing that does not change decisions, charging for visits that produce no plan. The rhythm itself is the most ethically clean model a precision practice can run, because every touchpoint is tied to a specific clinical purpose.
The Practice Economics, Made Concrete
A practice running the cadence cleanly on a full caseload of 40 to 60 active patients typically produces revenue distributed roughly as follows:
Testing and interpretation generates the first pillar — between a fourth and a third of gross revenue, depending on the practitioner's lab margins and whether they charge separately for interpretation. This is a predictable revenue stream because every patient in the cadence is either pre-testing or pre-retesting at any given moment.
Clinical visits — the protocol visits, the follow-ups, the mid-cycle check-ins — generate the second pillar, typically 35% to 50% of gross revenue. This is where the practitioner's time is most valuable and where pricing should reflect the depth of the work.
Supplementation margin — run through Fullscript or equivalent — generates the third pillar, typically 20% to 40% of gross revenue depending on practice model. This is the recurring layer that smooths cash flow across the month and underwrites the practitioner's time for the complex protocol work.
A practice running this cadence on forty patients, with clear pricing and consistent retesting, produces a genuinely sustainable practitioner income while serving a manageable caseload. A practice that never establishes the cadence must serve substantially more patients to produce the same income, which means less time per patient, which means the clinical work suffers, which means patients leave, which means the practitioner must recruit more new patients, which means less time for existing patients. The feedback loop runs the wrong direction.
Building the Cadence Into the Protocol From Day One
The practitioners who implement this cadence most reliably do one specific thing: they build the retest into the protocol before the patient leaves the first visit.
This sounds simple and is very rare in practice. The protocol document the patient receives specifies not only the testing, the interventions, the sequencing, and the timeline, but also the specific retest — which panels, at which week, with a scheduled appointment already on the calendar. The patient leaves knowing exactly what success will look like, when it will be measured, and what the next phase of work will be. This commitment device — a scheduled date, specific panels, clear endpoints — transforms retest follow-through from roughly 40% in most precision practices to above 80% in practices that have built it in from day one.
This is also one of the clearest places the Body MAX Harmonics BOTs earn their keep. The Individual Protocol BOT outputs a complete protocol document that includes the phased interventions, the sequencing, the retest cadence, and the specific panels to repeat — as standard architecture, not as an afterthought. The practitioner reviews, adjusts, and delivers. The cadence is built in by default, because the tool was built around the cadence.
One Practical Recommendation
If you are a precision practitioner reading this and recognizing that your cadence is not as tight as it could be, the intervention I would recommend is a single one.
Take your next five new patient intakes and, at the end of the protocol visit, put the retest appointment on the calendar before the patient leaves. Specify the panels. Tell the patient what you will be looking for. Send them home with a written protocol document that includes the retest at the top.
Do this for five patients. Watch what changes in your practice — in the follow-through, in the quality of the second visit, in the patient's engagement with the protocol in the intervening weeks, in your ability to tell whether the work is landing.
The cadence is not a marketing concept. It is a clinical discipline. But it is also, not coincidentally, the most reliable engine of a sustainable precision practice I have seen in two decades of this work. Build it into your next patient, and the one after, and the one after. In twelve months, the rhythm will have remade the economics of your practice from the inside.
Dr. Lily Woods, PhD is the founder of Body MAX Harmonics and the designer of the Woods Method protocol system. Body MAX Harmonics is a wellness education program for licensed and certified practitioners. Materials provided are wellness education frameworks applied at the discretion of the practitioner within their own scope of practice.