
Why Most Functional Medicine Protocols Fail the Precision Test
The uncomfortable truth about the gap between "functional" and "precise" — and what it will take to close it.
A Category Confusion That Costs Patients
Functional medicine and precision medicine are not the same thing. Somewhere in the last decade we started using the terms interchangeably, and our patients have been paying for that confusion ever since.
Functional medicine is a philosophy. It asks upstream questions. It treats the person rather than the diagnosis. It takes the microbiome seriously, the mitochondria seriously, the environment seriously. These are all good instincts, and they are the reason the field has grown.
Precision medicine is a method. It produces different protocols for different patients with the same presenting condition, calibrated to their specific biology as revealed by testing. It distinguishes between two patients with SIBO who require opposite interventions. It distinguishes between two patients with cognitive decline who share an ApoE genotype but have opposite metabolic phenotypes. It refuses to treat the category when the individual is what matters.
A functional protocol can be deeply unprecise. A precision protocol can be philosophically incoherent. In the best work, the two layer together — the functional philosophy asking the right questions, the precision method finding the right answers for this specific patient. In most of the work I see, they do not.
This essay is about why, and what it takes to do better.
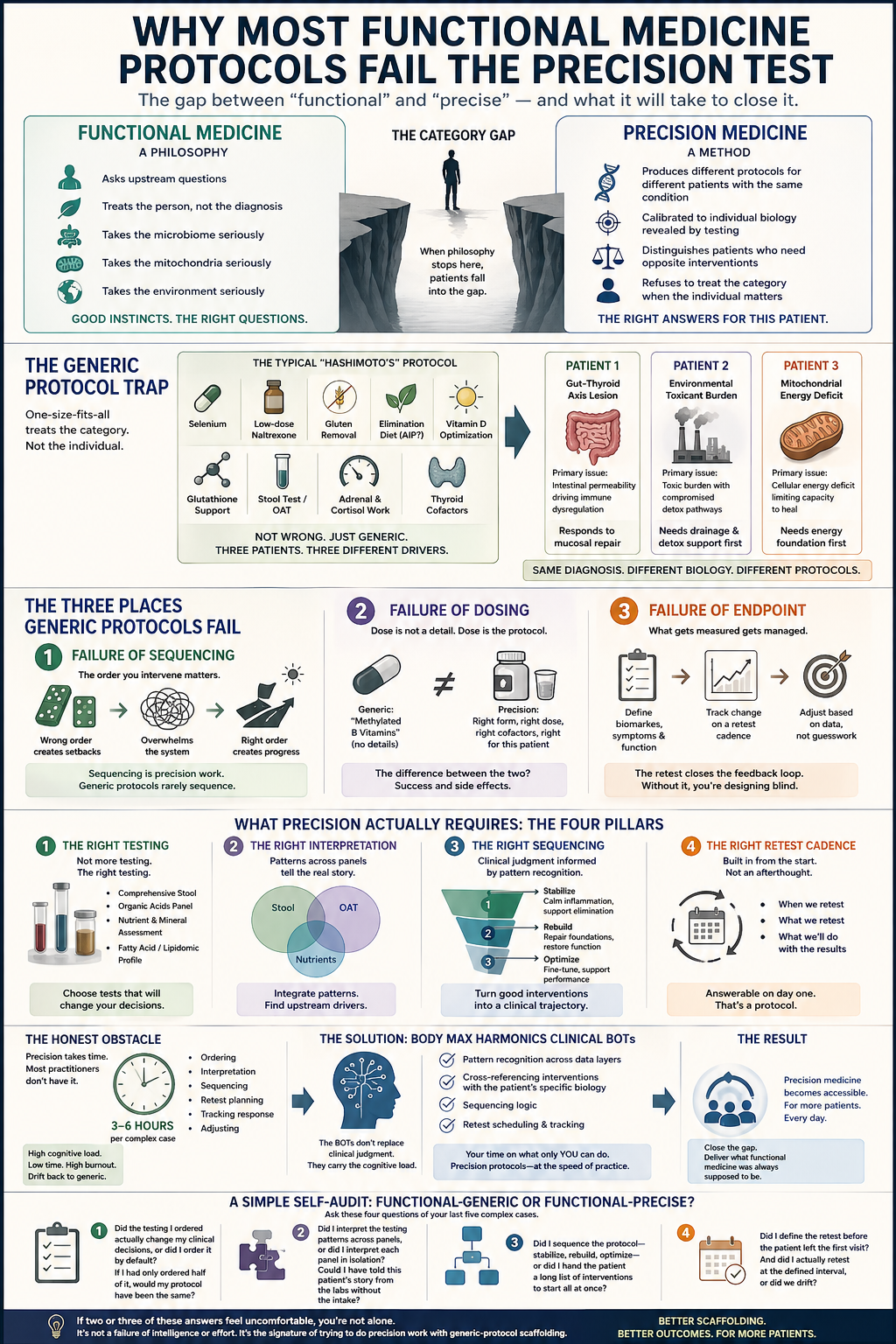
The Generic Protocol Trap
Walk into any functional medicine clinic and ask how they treat, say, Hashimoto's. You will get a recognizable answer. Selenium. Low-dose naltrexone, sometimes. Gluten removal. An elimination diet, maybe AIP. Vitamin D optimization. Glutathione support. A stool test, perhaps an organic acids panel. Some form of adrenal and cortisol work. Thyroid cofactors.
This is not wrong. Every piece of it has evidence behind it. Patients do get better on versions of this protocol, and the better practitioners have refined their version over years of practice.
But it is a generic protocol for a category of patients, not a precision protocol for an individual. Two patients with Hashimoto's may have entirely different biochemical drivers of their autoimmunity. One may have a primary gut-thyroid axis lesion — compromised intestinal permeability driving the immune dysregulation — and respond dramatically to mucosal repair. The other may have primary environmental toxicant burden, with gut dysfunction secondary, and fail to improve on any amount of gut protocol until drainage pathways and detoxification capacity are addressed. A third may have a mitochondrial energy deficit underneath it all, and simply cannot generate the metabolic work required to execute the protocol you designed.
The category "Hashimoto's" does not tell you which of those three patients is in front of you. The generic protocol treats them identically. The precision protocol treats them differently, because their biology is different.
The Three Places Generic Protocols Fail
When I audit protocols that have stalled — protocols designed by intelligent practitioners, for intelligent patients, with good tools and good intentions — the failure is almost always in one of three places.
The first failure is failure of sequencing. The order in which you intervene matters. Introducing aggressive microbiome work before mitochondrial capacity is sufficient produces a patient who feels worse, not better — because the body does not have the cellular energy to execute the die-off, the neurotransmitter shifts, the immune recalibration the protocol is demanding. Introducing detoxification before elimination pathways are ready produces toxin redistribution, not clearance. Introducing hormone support before the raw materials of steroidogenesis are available produces no change on the labs and a frustrated patient. Sequencing is precision work. Generic protocols rarely sequence because they are designed for a category, not an individual.
The second failure is failure of dosing. A generic protocol specifies "methylated B vitamins." A precision protocol specifies the form, the dose, and the cofactor environment based on the patient's MTHFR variants, their homocysteine, their B12 status, their current symptom set, and their tolerance. The difference between these two approaches is the difference between a patient who responds beautifully and a patient who develops the overmethylation symptoms that are now so common in functional medicine practice that they have become a sub-specialty unto themselves. Dose is not a detail. Dose is the protocol.
The third failure is failure of endpoint. How do you know the protocol is working? A generic protocol measures by symptom change. A precision protocol measures by biomarker change, symptom change, and functional capacity change, on a defined retest cadence. Without endpoints, protocols drift. Patients stay on interventions they should have stepped down from months ago. Practitioners cannot tell whether their work is landing. The retest is the closing of the feedback loop, and without it the practitioner is designing a protocol blind.
What Precision Actually Requires
Precision, in a clinical protocol, is the product of four things. A generic protocol has one or two of them. A precision protocol has all four.
First, the right testing — not more testing, the right testing. This is where most practitioners over-invest. You do not need seventeen panels on a first visit. You need the three or four panels that will change your clinical decisions. For most complex cases, that means a comprehensive stool panel with functional markers, an organic acids panel, a nutrient and mineral assessment, and a fatty acid or lipidomic profile. Hormone panels, genetic panels, metabolomic panels, mycotoxin panels are added based on clinical indication, not by default. The skill is choosing which tests will change what you do.
Second, the right interpretation — which is where most practitioners under-invest. Reading a functional panel well is a discipline. The patterns across a stool panel, an organic acids panel, and a nutrient panel tell a coherent story when you know how to read them. They reveal the upstream drivers in a way no single test does alone. This is the skill that separates the practitioner who "orders the DUTCH test" from the practitioner who actually knows what the DUTCH test is telling them when the dehydroepiandrosterone metabolites are low but the cortisol awakening response is elevated and the estrogen clearance is poor.
Third, the right protocol sequencing — which is clinical judgment informed by pattern recognition across thousands of cases. This is the hardest part to systematize, which is why most generic protocols do not attempt it. The sequence is what turns a collection of good interventions into a clinical trajectory.
Fourth, the right retest cadence — built into the protocol from the start. The question "when will we retest, and what will we retest, and what will we do with the results" should be answerable on day one of the protocol. If it is not, the protocol is not a protocol. It is a collection of recommendations.
The Honest Obstacle
Here is the part that usually goes unsaid. All four of these requirements are expensive in practitioner time.
Doing precision work correctly takes three to six hours per complex case — the ordering, the interpretation, the sequencing, the retest planning, the tracking of response, the adjustments. This is why precision medicine has historically been accessible only to patients who could afford high-priced practitioners, and why most practitioners, over time, have quietly drifted from precision back toward generic protocols. It is not an intellectual failure. It is an economic one. The cognitive load of doing this well is simply too high to carry across a full caseload.
This is the problem the Body MAX Harmonics clinical BOTs were built to solve. The BOTs do not replace the clinical judgment in any of the four requirements. What they do is carry the cognitive load — the pattern recognition across data layers, the cross-referencing of interventions against the patient's specific biology, the sequencing logic, the retest scheduling — so that the practitioner's time is spent on what only a practitioner can do. The result is not faster generic protocols. It is precision protocols that a working clinician can actually produce, repeatedly, across a full practice.
The category confusion between functional and precision medicine has been costing patients for years. The underlying gap is not philosophical. It is operational. When you give practitioners the scaffolding to do precision work at the speed of a normal clinical day, precision medicine stops being the rarefied thing it has become. It becomes what functional medicine was always supposed to be.
A Simple Self-Audit for Your Own Protocols
If you want to test whether your own protocols are functional-generic or functional-precise, ask these four questions of your last five complex cases:
Did the testing I ordered actually change my clinical decisions, or did I order it by default? If I had only ordered half of it, would my protocol have been the same?
Did I interpret the testing patterns across panels, or did I interpret each panel in isolation? Could I have told this patient's story from the labs without the intake?
Did I sequence the protocol — stabilize, rebuild, optimize — or did I hand the patient a long list of interventions to start all at once?
Did I define the retest before the patient left the first visit? And did I actually retest at the defined interval, or did we drift?
Most practitioners who run this audit honestly find that two or three of those answers are uncomfortable. That is not a failure of intelligence or effort. It is the signature of trying to do precision work with generic-protocol scaffolding. The scaffolding is the problem worth solving.
Dr. Lily Woods, PhD is the founder of Body MAX Harmonics and the designer of the Woods Method protocol system. Body MAX Harmonics is a wellness education program for licensed and certified practitioners. Materials provided are wellness education frameworks applied at the discretion of the practitioner within their own scope of practice.