
Why two people with the same health problem may need different protocols.
Conventional care sorts patients into disease states and matches each to a standard of care. That system is not wrong — but it stops one layer short of the individual biology that decides how a given person's systems actually run. Here is the evidence for that layer, and why reading it is a learnable clinical skill.
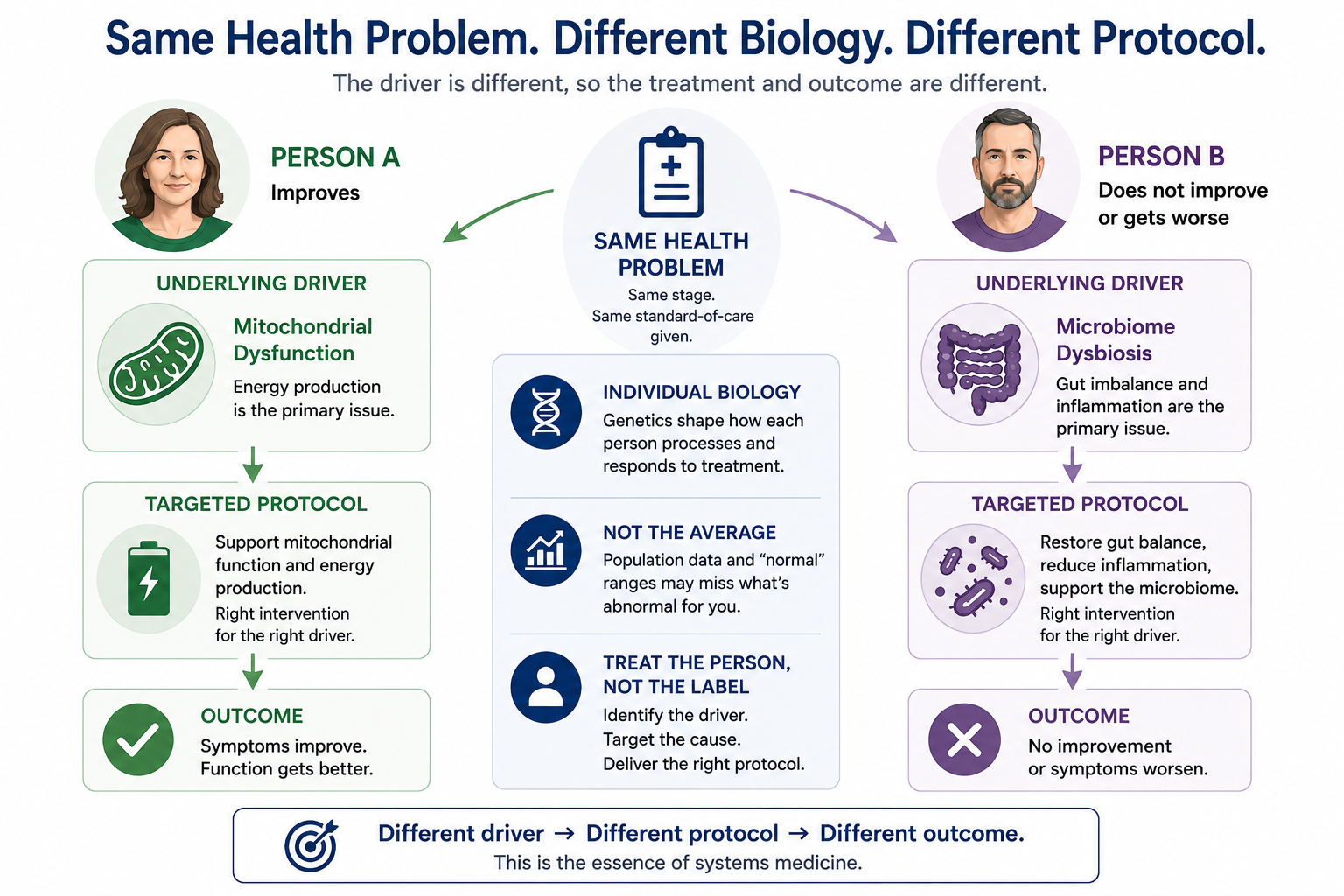
A practitioner sees two patients in one afternoon. Same diagnosis, same stage, same standard-of-care protocol. One improves. One does not — or gets worse. Nothing in the chart explains the divergence, because the thing that explains it was never on the chart. It sits one layer beneath the diagnosis: the individual biology that determines how each person's systems process the very intervention they were both given.
This is the premise of systems medicine, and it is not fringe. It is the direction the field has been moving for two decades. Leroy Hood and colleagues framed it as P4 medicine — predictive, preventive, personalized, and participatory — grounded in the recognition that disease emerges from perturbed biological networks that differ from person to person, and that treating the network rather than the label is where medicine is headed.[1] The Woods Method is a structured, teachable way of doing exactly that: reading the individual layer first, then letting the treatment go where that person's biology points.
The problem with treating the average
A standard of care is, by construction, an average. It is the intervention that produces the best outcome across a population of people who share a diagnosis. That is a genuine achievement, and for many patients it works. But an average is not a person. The moment you apply a population-derived protocol to an individual, you are making a bet that this person resembles the average closely enough — in how they metabolize, clear, methylate, absorb, and respond — for the average answer to be the right one for them.
Often that bet is fine. Sometimes it is merely suboptimal. And sometimes it is wrong in a way that harms, because the same dose that is therapeutic for the average is an overdose for the person whose clearance is genetically slow. The difference between those three outcomes is not visible in the health problem. It is visible only in the individual — if you know to look, and know what you are looking at.
Name the pathway, and the protocol fits the person
Two patients carry the same diagnosis and are driven by entirely different terrain. One presentation is downstream of mitochondrial insufficiency; another of microbiome dysbiosis; another of membrane and lipid biology; another of toxic and inflammatory burden. The label is the same. The driver is not. And the driver is what a protocol has to target if it is going to do anything but chase symptoms.
Each of these drivers is a mature field of evidence in its own right. Mitochondrial dysfunction is now recognized not as a niche concern but as a shared mechanism beneath neurodegenerative disease, cardiovascular disease, and age-related metabolic disorders — an energy supply-and-demand imbalance that expresses differently in different people.[2] Gut microbiome dysbiosis is likewise established as a pathological basis for a wide range of conditions, with host genetics and environment shaping which individuals are susceptible and how their dysbiosis manifests.[3] The point is not that one of these is the master key. The point is the opposite: which one is driving a given presentation is an individual question, and the method's job is to identify it rather than apply a favorite lens to everyone.
This is what the Four Horsemen, the Four Hingepins, and the Six Pathway System are built to make repeatable — a structured way to reason from the presentation to the actual driver, so the protocol targets the cause in this person rather than the label they share with a thousand others.
Genetics sit beneath the pathways
Underneath the pathways is the layer that governs how a person handles any intervention at all: their genetics. This is the part of the argument where the evidence is not merely suggestive but quantitative, and where the harm case is most concrete.
Consider drug metabolism. The cytochrome P450 enzymes handle the biotransformation of most clinical drugs, and the genes encoding them are highly polymorphic. For CYP2D6 alone, genetic variation can require up to a tenfold difference in dose to reach the same plasma concentration between two individuals.[4] This is not a laboratory curiosity. In one pharmacokinetic study, children given the identical weight-adjusted dose of the same medication showed thirty- to fiftyfold differences in drug exposure, with the highest concentrations in those genetically deficient in the metabolizing enzyme. The same prescription was a reasonable dose for one child and a massive overexposure for another — distinguishable in advance only by genotype.
The same principle runs through phase-two metabolism and methylation. Glutathione S-transferases carry out a large share of the body's detoxification of electrophilic compounds and products of oxidative stress; common null genotypes in GSTM1 and GSTT1 result in partial or complete loss of that enzyme activity, leaving affected individuals measurably less able to clear the load.[5] In folate metabolism, the MTHFR C677T variant produces a thermolabile enzyme; each copy of the risk allele lowers activity by roughly a third, so that homozygous individuals operate at around a quarter of typical enzyme activity, with downstream effects on methylation and homocysteine.[6] Sulfur handling, methylation capacity, detoxification throughput — each is one more axis on which two people who look identical on paper are not identical in what a given intervention will do inside them.
None of these is the centerpiece. That is precisely the point. The method does not lean on a favored gene or a favored pathway. It leans where the individual's biology requires it to lean — and the clinical skill is knowing which axis matters for the person in front of you.
Even the labs mislead without the individual picture
There is a quieter version of this problem that trips up even careful clinicians, and it lives in the reference ranges on every lab report. Those ranges are population-derived: they describe where results fall across a population of ostensibly healthy people (and in the US, unhealthy). But an individual's own healthy range — the interval their body actually holds a marker within — is typically far narrower, and occupies only a small slice of the population range.
The formal expression of this is the index of individuality, the ratio of within-person to between-person biological variation. For most markers that ratio is low, which means population reference intervals are of limited use for judging an individual: a result can sit comfortably inside the "normal" band and still be distinctly abnormal for that person.[7] A modern modeling study made the consequence concrete: when personalized reference intervals were computed for a cohort, each person's interval differed from the next, and though every one sat within the common population range, in general it made up only a small proportion of it.[8] A real signal, in other words, read as noise — because it was measured against the average instead of against the person.
This is why the individual picture is not a luxury layered on top of good medicine. Without it, the data itself can point the wrong way.
Why this is a teachable skill
It would be easy to read all of this as an argument for complexity — for treating every patient as an irreducible mystery. It is the opposite. The individual layer is not chaos; it is structured, and the structure can be taught. Knowing that CYP metabolizer status changes exposure, that detoxification capacity varies with genotype, that a marker's meaning depends on the person's own set point rather than the population's — these are learnable, applicable, repeatable ways of reasoning. That is what a framework is for.
The Woods Method certification teaches this reasoning as a discipline: how to move from a presentation to the pathway actually driving it, how to account for the genetics running beneath, and how to read the individual rather than the average. It is the difference between a protocol that is merely generic and one that is right for the person in front of you — and, at times, the difference between one that helps and one that harms.
Learn to read the layer beneath the diagnosis.
The Core Pathway Certification teaches the reasoning in this article as a structured clinical discipline — assessed against primary literature, built for practitioners who want to treat the individual rather than the average.
References
Hood L, Flores M. A personal view on systems medicine and the emergence of proactive P4 medicine: predictive, preventive, personalized and participatory. New Biotechnology, 2012;29(6):613–624.
Amorim JA, et al. Mitochondrial and metabolic dysfunction in ageing and age-related diseases. Nature Reviews Endocrinology, 2022;18(4):243–258.
Shen Y, et al. Gut microbiota dysbiosis: pathogenesis, diseases, prevention, and therapy. MedComm, 2025;6(4):e70168.
Zanger UM, Schwab M. Cytochrome P450 enzymes in drug metabolism: regulation of gene expression, enzyme activities, and impact of genetic variation. Pharmacology & Therapeutics, 2013;138(1):103–141.
Hayes JD, Flanagan JU, Jowsey IR. Glutathione transferases. Annual Review of Pharmacology and Toxicology, 2005;45:51–88.
Frosst P, et al. A candidate genetic risk factor for vascular disease: a common mutation in methylenetetrahydrofolate reductase. Nature Genetics, 1995;10(1):111–113.
Fraser CG. Biological variation: a rapidly evolving aspect of laboratory medicine. Journal of Laboratory and Precision Medicine, 2017;2:35.
Coşkun A, et al. Personalized reference intervals in laboratory medicine: a new model based on within-subject biological variation. Clinical Chemistry, 2021;67(2):374–384.
This article is a clinical education briefing for practitioners and is not medical advice. Clinical and dosing decisions require appropriate professional judgment and oversight.